
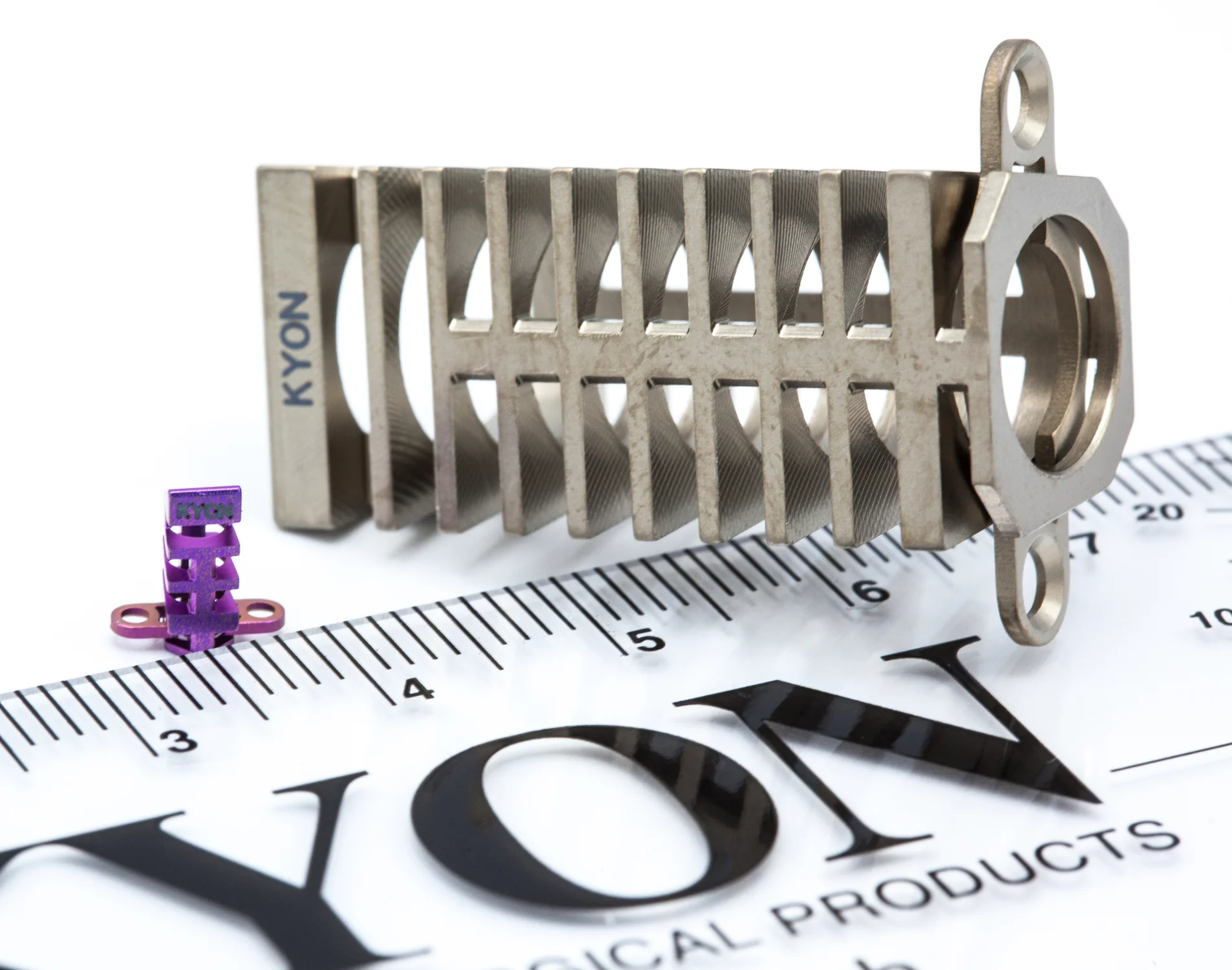
KYON TTA-2 – Tibiala Tuberosity Advancement
TTA-2 is a second generation device for the TTA procedure that delivers the TTA outcomes with less trauma, fewer implants, a simplified technique and at a reduced cost.

TTA-2 is even less invasive than TTA as it requires smaller and fewer holes in the tibia.
Simplified technique through fewer implant parts. Stapling removes the need for screws.
Economic solution through reduced capital and carrying cost
Clinically proven
- Over 4 years of clinical study and 700 cases performed.
- Since launch, more than 6,000 cases have been performed.

In early 2004, KYON launched TTA for cranial cruciate deficiency in dogs following three years of clinical testing. The rapid acceptance of TTA has motivated several other companies to offer similar implants. The TTA technique was developed on the basis of systematic observation and simple biomechanical analysis of the canine knee.
TTA is designed to be less invasive than other geometry modifying techniques such as TPLO when treating the most common cause of lameness in dogs.
TTA does not change the joint geometry. It neutralizes cranial tibial thrust in cranial cruciate deficient stifles and thus decreases internal joint reactions by a sound biomechanical rationale.
Reduced post-surgical complications and accelerated recovery through:
- A broad range of sizes: more than 30 different cage sizes available
- Extra long shape, providing a better fit and easier cut, ideal for skinny tibia breeds
- Superb biocompatibility through titanium material

Execution
The TTA involves an osteotomy of the non-weight bearing portion of the tibia. The patellar ligament is aligned perpendicularly to the common tangent of the femorotibial joint, eliminating cranial tibial thrust. This new alignment eliminates the need for the CrCL and results in a stable joint.
- The required advancement of the patellar ligament insertion at the tibial tuberosity is measured from a radiograph of the stifle in extension.
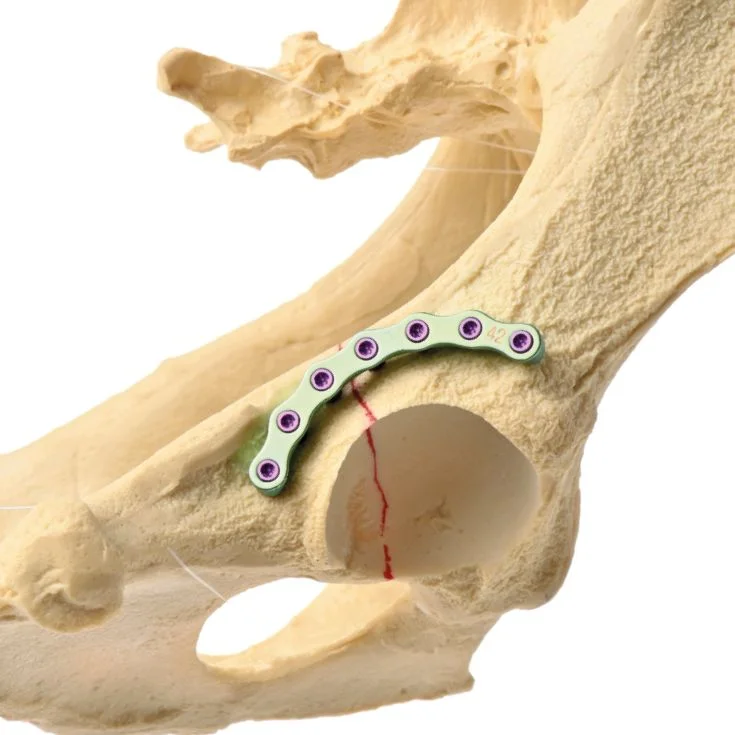
- With a frontal plane osteotomy, the tibial tuberosity is advanced and held in position by:
(1) A cage transferring the compression component of the patellar ligament force from the tuberosity to the proximal tibia
(2) A tension band plate transferring the patellar ligament force to the proximal diaphysis of the tibia
- The open osteotomy, distal to the cage, is grafted with autologous cancellous bone or other graft material such as allograft or hydroxyapatite (HA) to accelerate healing.

Principles
The TTA technique was developed on the basis of systematic observation and simple biomechanical analysis of the canine knee joint:
- Total joint force in the stifle is approximately parallel to the patellar ligament
- If the angle between the patellar ligament and the common tangent at the tibio-femoral point of contact (call it alpha) is 90 degrees, neither of the cruciates is loaded.
- In the canine stifle, alpha is 90 degrees at 110 degrees of flexion (call this a crossover flexion point). In full extension (approximately 135° stifle angle) alpha is approximately 105 degrees. In full flexion it is approximately 80 degrees.
- With the stifle in extension with respect to the crossover point, the load is on the cranial cruciate ligament. With the stifle flexed past the crossover point, the load is on the caudal cruciate ligament.
- With the cranial cruciate ligament gone, the stifle can be stabilized by shifting the crossover point to the full extension.
- This can be done by either TPLO (turning the plateau) or by TTA (advancing the patellar ligament).
Whitepaper
Download the following whitepaper, to learn more about
- TTA’s history and rationale
- Do’s and Don’ts in preoperative planning
- Important steps in the technique to improve outcomes.